
What is - Neurovascular
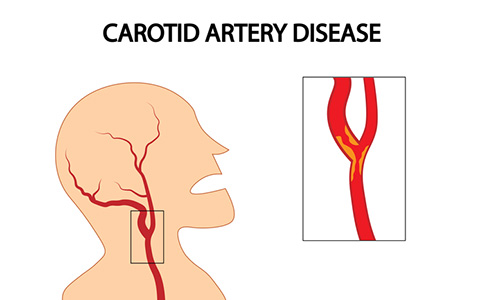
Carotid Artery Disease
In Singapore, stroke is the 4th leading cause of death and a major contributor to long term disability. A stroke or "brain attack" can occur when one of the major arteries in the neck (the carotid artery) is narrowed by fatty deposits (plaques). This results in carotid artery disease simillar to coronary heart disease. Such "hardening" of the carotid artery can lead to damage to part of the brain, either as a consequence of reduced blood flow or because small pieces of "emboli" break off from the plaque and lodge into arteries in the brain or eye. This ultimately results in an ischaemic type of stroke, which accounts for 75% of all strokes.
Symptoms of Neurovascular
There may not be any symptoms of carotid artery disease. However, there are warning signs of a stroke. A transient ischemic attack (also called TIA or "mini-stroke") is one of the most important warning signs of a stroke. A TIA is a temporary episode of:
- Blurred or loss of vision in one or both eyes
- Weakness and/or numbness of your arm, leg or face on one side of your body
- Slurring of speech, difficulty talking or understanding what others are saying
- Loss of coordination, dizziness or confusion
- Trouble swallowing
Neurovascular - Causes and Risk Factors
The risk factors for carotid artery disease is similar to those for coronary artery disease:
- Family history of atherosclerosis (either coronary artery disease or carotid artery disease)
- Age (greater in men than women less than age 75, but higher in women after age 75)
- Smoking
- Hypertension
- Diabetes
- High low density lipoprotein (LDL, bad cholesterol) - although this link is not as strong as it is for coronary artery disease
Diagnosis of Neurovascular
The following are tests carried out to confirm the diagnosis of carotid artery disease.
Carotid Duplex Ultrasound
An imaging procedure that uses high-frequency sound waves to view the blood vessels in the neck and to determine the presence of narrowing in the carotid arteries. This study is recommended in anyone with heart disease and anyone over the age of 60.
Carotid Angiography
This is a procedure to image the carotid artery. It can be done via a specialised CT scan (CT Angiography) , MRI scan (MR angiography) or via a catheter angiogram. This is an invasive imaging procedure that involves inserting a catheter into a blood vessel in the arm or leg, and guiding it to the carotid arteries with the aid of a special x-ray machine. Contrast dye is injected through the catheter so that x-rays of your carotid arteries are taken.
Treatment for Neurovascular
Carotid Endarterectomy
Carotid endarterectomy (CEA) is a surgical procedure performed to reduce the risk of stroke in patients with significant carotid artery disease. This procedure does not apply to haemorrhagic strokes (bleeding in the brain), which make up the other 25% of strokes. The surgery to remove this narrowing in the carotid artery can help prevent a stroke. However, it cannot improve the outcome of a stroke that has already occurred. CEA is more effective than medical management in the prevention of stroke. However, this is true for certain groups of patients under defined circumstances.
In patients with symptomatic and severe disease of >70-99%, such as patients with symptoms of stroke, transient ischaemic attack (TIA or mini-stroke) or amaurosis fugax (transient blindness) due to carotid artery narrowing of >70-99%, CEA has significant benefit over medical management. The risk-benefit ratio favors surgery only if the perioperative morbidity and mortality is <6%.
Patients with asymptomatic disease and carotid artery stenosis of >60%, such as patients with carotid artery narrowing of >60% but who experience no symptoms, benefit substantially less from CEA. For any benefit at all, surgery must be performed at very low stroke rates, in the range of 2-3%.
In symptomatic severe carotid artery narrowing, several trials have shown CEA to be superior to medical management for the prevention of stroke. The North American Symptomatic Carotid Endarterectomy Trial (NASCET), published in 1991, showed a significant benefit for CEA in patients with severe carotid artery stenosis of >70% demonstrated on angiography. In the NASCET trial, CEA resulted in an absolute risk reduction of stroke by 17% at 2 years. This difference in outcome between medical therapy and surgery plus medical therapy represented a relative risk reduction of 65%. Thus, surgery was beneficial for persons with severe carotid artery narrowing and who had experienced a stroke or its warning signs. The European Carotid Surgery Trial (ECST), published in 1991, also demonstrated a similar benefit in such patients with severe carotid artery stenosis. It is important to realise that the perioperative stroke and death rate has to be <6% for CEA to be effective.
CEA has been shown to be beneficial in patients without symptoms but this benefit is less substantial. The Asymptomatic Carotid Atherosclerosis Study (ACAS), published in 1995, is the largest and most definitive randomised trial that evaluated the efficacy of surgery in patients with severe stenosis of >60% detected by ultrasound. The 5-year projected risk of stroke was reduced by surgery from 11% to 5.1%. While this is translated to a relative risk reduction of 53%, the absolute risk reduction at 2 years was only 1.5% (meaning that 67 patients would need to undergo surgery to prevent one non-disabling stroke). Furthermore, surgery did not protect against major stroke and death and the results were not significant when women were analysed as a discrete population. With a modest benefit of surgery in patients were severe stenosis and no symptoms, carotid endarterectomy is not routinely recommended. It should be only considered as a management option by surgeons with very low complication rates of <3% in the presence of other high risk factors (eg, stenosis of the opposite carotid artery, plaque ulceration etc). Medical management is a sensible alternative for most of such patients.
The surgery involves a skin incision is placed obliquely across the side of the neck. The branches of the artery and the carotid artery before and after the site of narrowing are clamped and an openning is then made over the area of narrowing. The plaques causing the narrowing are removed and the openning is repaired with very fine sutures.
The potential risks for this procedure are as listed:
- Stroke: Interruption of blood supply during surgery can potentially cause permanent damage to the brain
- Heart attack: Because of a high incidence of coexistent cardiac disease and hypertension, this can also occur
- Neck haematomas: This can be life-threatening especially if it compromises breathing. Breakdown of the arteriotomy repair is uncommon but can be fatal. Occasionally, bleeding at the operation site may involve re-opening of the wound
- Skin numbness
- Wound infection
- Injury to surrounding structures such as the hypoglossal nerve which controls movement of the tongue
Contributed by
The information provided is not intended as medical advice. Terms of use. Information provided by SingHealth.
Our Medical Specialists
1
2
3
4
5
Health Articles

Stay Healthy The Easy Way
Get trusted health advice, offers and more.
Stay Ahead in Healthcare Industry
Subscribe to our exclusive updates for healthcare professionals.










Keep Healthy With
Follow SingHealth




© 2025 SingHealth Group. All Rights Reserved.